
machines that make medicine
hello and welcome to the future of pharma. machines make medicine now. here's what it looks like

Panoptic Bio is building a vertically integrated AI pharma company for the new era. Agent-run clinical trials, connected directly to automated biomanufacturing.
Agent-run clinical trials
Each year, the world spends $1.7T on existing pharmaceuticals and $276B on new pharmaceutical R&D.1 The pharmaceutical development cycle is as follows:
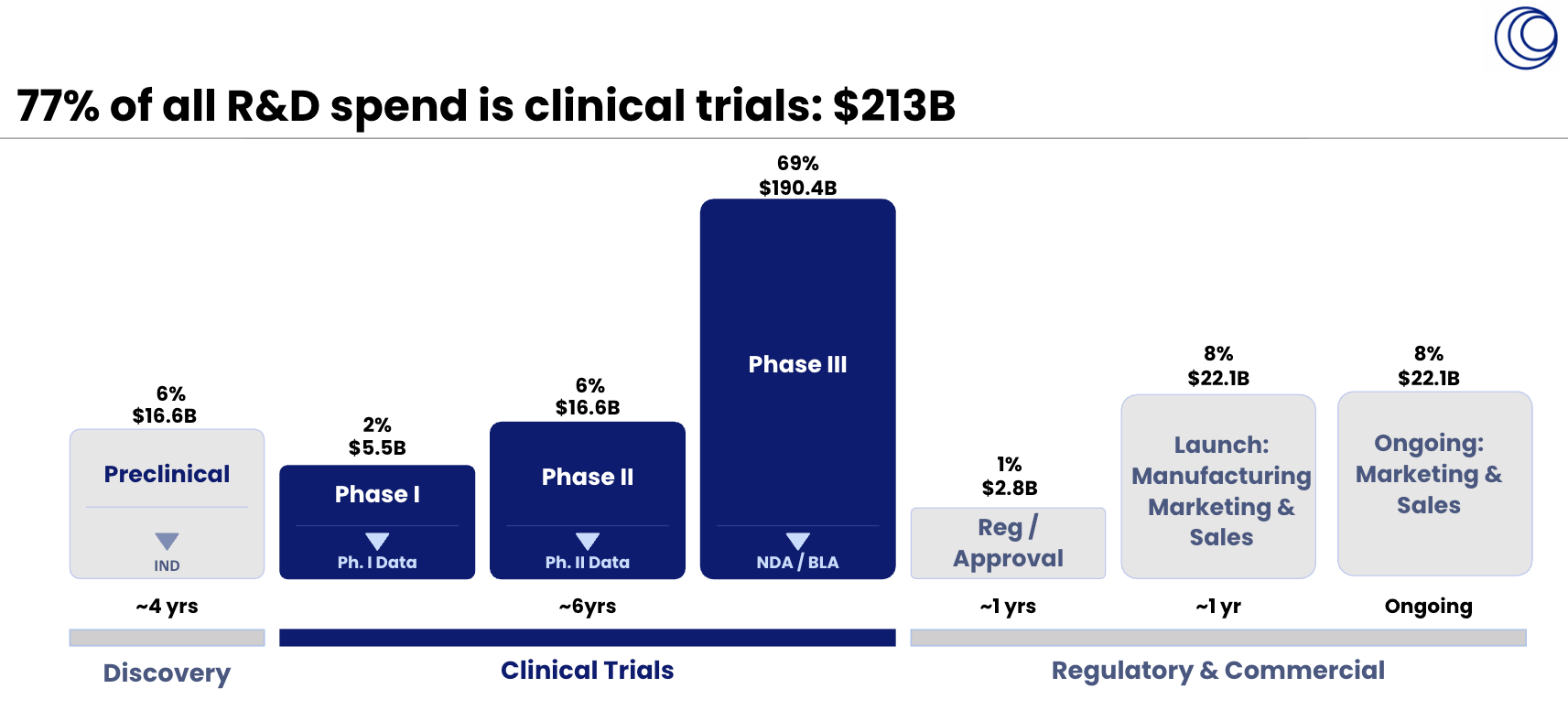
A new drug spends an average of 4 years in discovery, 6 years in clinical trials, and 1 more year to reach market. Most of the time and money the industry spends is in clinical trials. Yet there is a big problem:
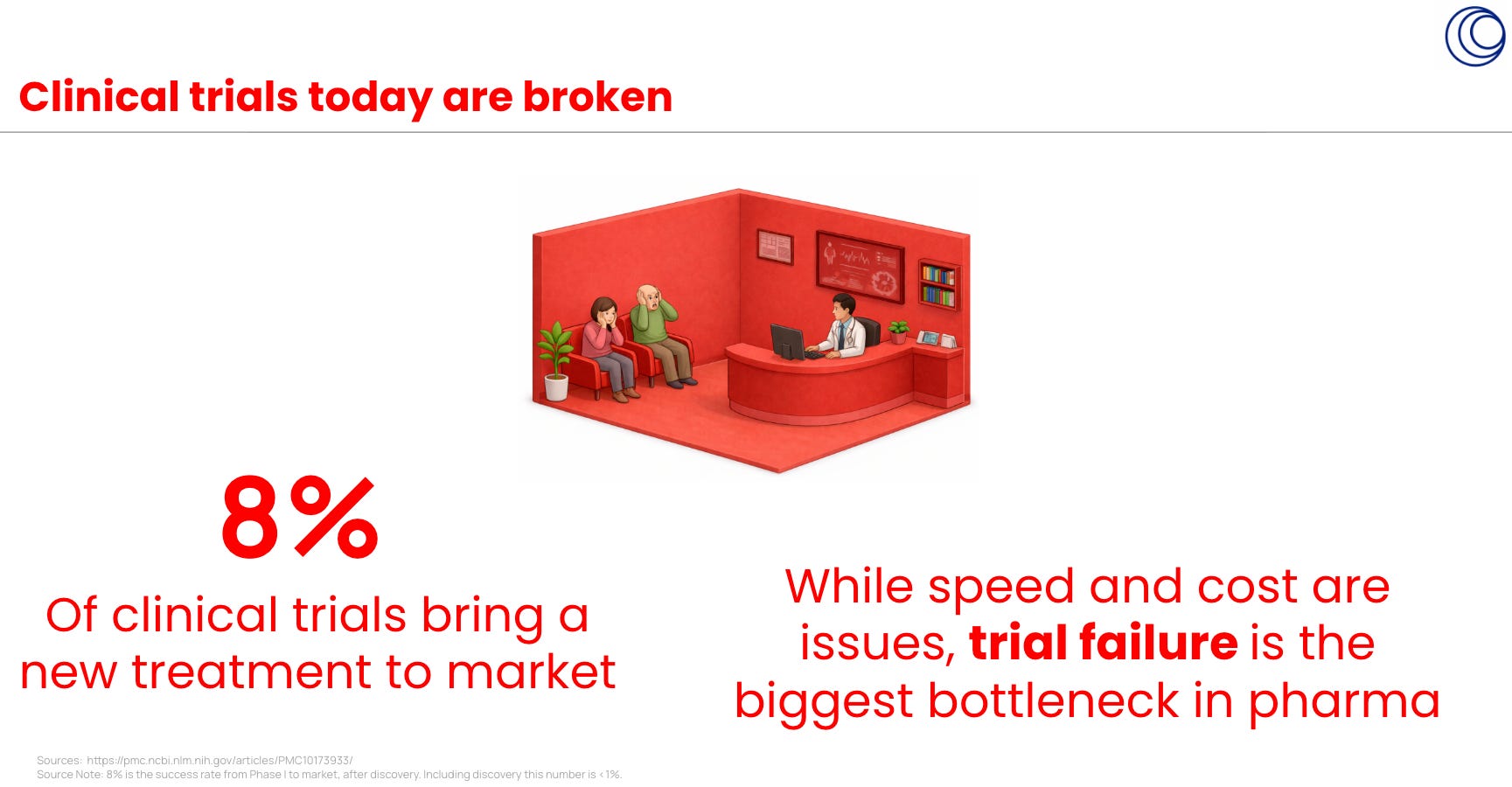
Clinical trial spend is ~$213B of that R&D spend and yet only 8% of drugs make it to market.
Digital AI, in the form of clinical trial intelligence, is already changing this.
In 2026, a team of Stanford researchers created an AI-agent system that can perform parts of pharma R&D,2 from target analysis to clinical-trial reasoning.
And in 2026, Panoptic Bio achieved the highest recall on clinical trial outcome prediction benchmarks.
At this current trend of Agent-led R&D in pharma, the industry will significantly transform over the next 10 years:

A suite of agents will execute the clinical trial workflow. Research agents quantify risk, create an integrated view across the clinical, commercial, and regulatory trajectory of a drug in trials, and humans will oversee this research before it is handed over to agents executing protocol writing, trial enrollment, patient dosing, statistical analysis, and regulatory submission.
The results will be an incredible win for humanity:
That research agent team who analyzes, integrates, and quantifies the clinical, commercial, and regulatory trajectory of a new drug through trials is what Panoptic Bio has built in our Trial Terminal:
Automated biomanufacturing
Machines will also make medicine.
After Digital AI and its R&D agents, Physical AI and automated biomanufacturing are next in the development lifecycle.
Agents will execute the clinical trial workflow digitally, and run into physical world barriers for the remainder of pharma R&D. Lab validation, pipetting, dosing mice, patient dosing in clinic, and manufacturing all require humans at the moment. And humans introduce error.
To make a drug reliably, at clinical grade, under significant regulation, and at scale, is difficult. Many human hands exist. CDMOs, suppliers, quality and control teams, manufacturing sites in India and China, and many, many consultants. Every handoff from one human hand to another adds time, cost, coordination risk, and human error.
Panoptic Bio is building a vertically integrated model where clinical intelligence connects directly to automated biomanufacturing. Trial agents identify the right indication, protocol, patient population, dosing regimen, and regulatory path, while manufacturing agents prepare the physical execution layer: process development, batch records, quality checks, release testing, supply planning, and clinical-grade production. Automated facilities will produce small molecules and biologics at scale, and the drug quality will be safer than human hands can make. (Just like how self driving became safer than human driving).
Clinical trials and manufacturing are not separate systems. They are one loop. They should exist in one company. Vertically integrated. In one building.
Made in America
America desperately needs a pharma infrastructure upgrade. Health has stagnated and the age of mortality has decreased in recent years.
Even though America launched the modern pharma and biotech industries, most drugs are now made through supply chains concentrated in India and China. The chemical inputs and APIs behind, in particular, almost all trace back to China. Amongst those biologics and advanced therapies that are still made in the West, it is done through fragmented CDMO networks relying on expensive human labor.
While many think that China is leveraging lower cost labor, the manufacturing capacity is largely automated. A combination of advanced robotics, automation, and industrial policy is China’s secret sauce for building the physical infrastructure for the next era of medicine.
America needs a new model. An AI-native pharma company that connects agent-run clinical trials directly to automated domestic biomanufacturing.
Can you imagine we made our own medicine in San Francisco?

This is how America maintains its edge in bio. A big bet on digital AI for clinical trials, physical AI for manufacturing, combined with industrial policy to upgrade our pharma infrastructure for the 21st century.
Made on Earth, for life in Space
Earth needs this pharma infra upgrade first. After all, this is where we all live. But the end-state idea is not limited to our home planet. This pharma infra upgrade should be built to be taken to-go, up to space.

Making medicine locally, automatically, and on demand using digital ai and physical ai, will set humanity up for successful astropharmacy. This Earth-based pharma infra that lets us run agent-led trials and manufacture drugs in-house is also the infrastructure needed for austere environments, such as lunar bases or Martian colonies. We’re building it on Earth first, and one day it will be the pharma infra needed to sustain eventual human colonies in space.3
The Big Bet
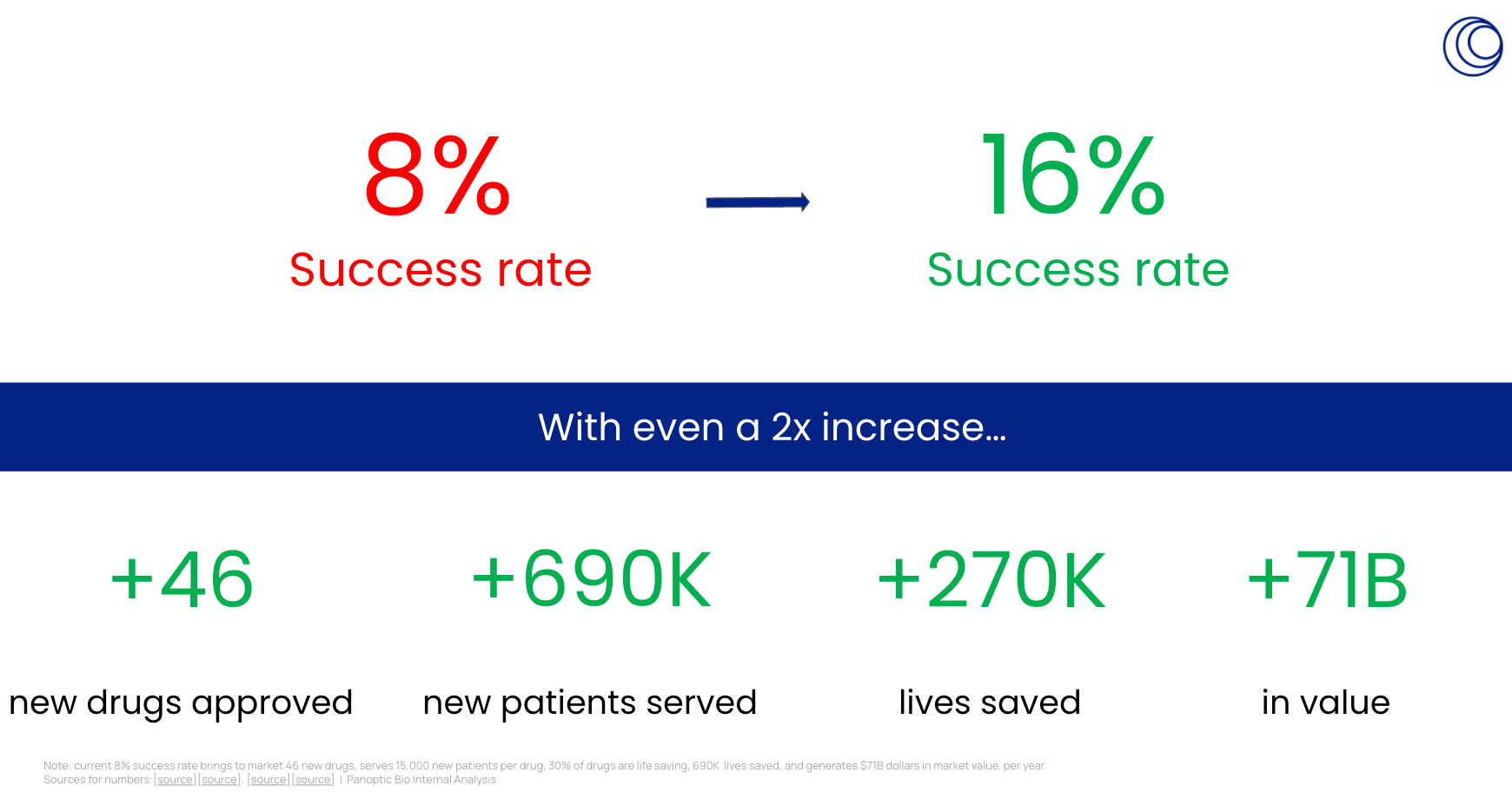
No opportunity is bigger for human health. A doubling of clinical trial success rates will bring 46 new drugs to market, serve >690K new patients, and save >270K additional lives each year. Making those drugs in America with automation is the only way to make them affordable for Americans.
And no industry is more ripe for disruption than pharma. Another B2B SaaS is not what they are going to buy, especially now that the even the senior pharma executive can claude-code! Rather than serving dinosaurs, it is time to build afresh.
As of 2026, Panoptic Bio is an early moonshot. But if it works, Panoptic Bio would transform pharma the way Spacex transformed aerospace.
Panoptic Bio
Machines the make medicine
www.panoptic.bio

What medicines work?
Learn about digital ai in pharmaceutical clinical trials: www.clinicaltrials.bio
How to make medicine?
Learn about physical ai in pharmaceutical manufacturing: www.manufactured.bio
What is Panoptic Bio’s company culture like?
Learn about how we work: www.opensourcetheculture.substack.com
Who is the Founder/CEO, Sebastian De Beurs?
www.sebastiandebeurs.com
Sources for article:
IQVIA Institute for Human Data Science. “The Global Use of Medicines 2024: Outlook to 2028.” January 2024. iqvia.com
Evaluate Ltd. “Evaluate Releases 2030 Forecasts for Global Pharmaceutical Market.” Press release, 2024. evaluate.com
Wong, Siah & Lo. “Estimation of Clinical Trial Success Rates.” Biostatistics, Vol. 20, Issue 2, April 2019, pp. 273–286. doi.org/10.1093/biostatistics/kxx069
Citeline. “Pharma R&D Annual Review 2024.” Citeline Intelligence, 2024. citeline.com/en/pharma-rd
U.S. National Library of Medicine. “ClinicalTrials.gov: A 25-year journey to a half-million registered studies.” NLM Director’s Blog, April 2, 2025. nlmdirector.nlm.nih.gov
U.S. Food and Drug Administration. “Novel Drug Approvals for 2024.” FDA Center for Drug Evaluation and Research. fda.gov/drugs/novel-drug-approvals-fda/novel-drug-approvals-2024
Alvarez, Daniel, et al. “Biopharma Trends 2026.” BCG Global, 8 Jan. 2026, www.bcg.com/publications/2026/reimagining-business-models-biopharma-trends.
Baedeker, Mathias, et al. “2023 FDA Approvals: Unprecedented Volume at Moderate Value.” Nature News, Nature Publishing Group, 17 Jan. 2024, www.nature.com/articles/d41573-024-00011-9.
DiMasi, Grabowski & Hansen. “Innovation in the Pharmaceutical Industry: New Estimates of R&D Costs.” Journal of Health Economics, Vol. 47, May 2016, pp. 20–33. doi.org/10.1016/j.jhealeco.2016.01.012
EY. “EY 2025 Biotech Beyond Borders Report.” June 2025. ey.com/en_us/newsroom/2025/06/ey-2025-biotech-beyond-borders-report-biopharma
Bessemer Venture Partners. “State of the Cloud 2024.” Bessemer Venture Partners, 2024. bvp.com/atlas/state-of-the-cloud-2024
Veeva Systems. “Annual Reports and SEC Filings (10-K, 2014–2024).” Veeva Systems Inc. SEC EDGAR.
EY. “Life Sciences M&A Spending Accelerates as the Industry Faces Growth Gaps.” EY Global, January 2026. ey.com/en_gl/newsroom/2026/01
“Global Pharma R&D Returns Rise as GLP-1 Drugs Help Drive Forecast Growth | Deloitte UK.” Deloitte United Kingdom, Deloitte, 25 Mar. 2025, www.deloitte.com/uk/en/about/press-room/global-pharma-rd-returns-rise-as-one-glp-drugs-help-drive-forecast-growth.html.
Mullard, Asher. “2025 FDA Approvals.” Nature Reviews Drug Discovery, 2 Jan. 2026, www.nature.com/articles/d41573-026-00001-z, https://doi.org/10.1038/d41573-026-00001-z.
Kim E, Yang J, Park S, Shin K. Factors Affecting Success of New Drug Clinical Trials. Ther Innov Regul Sci. 2023 Jul;57(4):737-750. doi: 10.1007/s43441-023-00509-1. Epub 2023 May 11. PMID: 37166743; PMCID: PMC10173933., https://pmc.ncbi.nlm.nih.gov/articles/PMC10173933/
Roden, Brian. The Staggering Cost of Drug Development: A Look at the Numbers – GreenField Chemical Inc. 10 Aug. 2023, greenfieldchemical.com/2023/08/10/the-staggering-cost-of-drug-development-a-look-at-the-numbers.
Footnotes:
IQVIA, Global Use of Medicines 2024 ($1.7T); PhRMA Annual Report 2024 ($246B global R&D); NLM/ClinicalTrials.gov April 2025 (500,000+ studies).
Note: $1.7T represents all spending by patients, physicians, hospitals, insurance, governments on treatments; $276B represents all clinical trial and drug development expenditure by biotech, pharma, and government
https://www.biorxiv.org/content/10.64898/2026.02.23.707551v1?utm=
https://ntrs.nasa.gov/citations/20250009075?utm=